A molecule released by the skin, lungs and gut is changing how scientists think about allergy, not simply as an overreaction of immune cells, but as a disease that may begin at damaged biological borders and reverberate throughout the body
A grain of pollen lands on the moist surface of an airway. A dust mite protein settles into microscopic cracks in inflamed skin. A respiratory virus infects the cells lining a bronchial tube. None of these encounters begins in the bloodstream or deep inside a lymph node. They begin at a border.
The human body has several such borders: the skin, the respiratory tract and the gastrointestinal tract. Together, these enormous surfaces form the interface between our internal biology and an environment crowded with microbes, foods, pollutants, allergens and chemicals. For decades, these tissues were often described mainly as barriers, walls that kept dangerous things out.
But a wall does not explain what happens next. Epithelial cells, the cells that form these borders, are increasingly understood as active sentinels. They sample their surroundings, detect injury and communicate with the immune system. When disturbed, they can release powerful signaling molecules capable of shaping inflammation long before the familiar hallmarks of allergy, IgE antibodies, activated mast cells, wheezing or itching, become apparent.
Among the most influential of these signals is thymic stromal lymphopoietin, better known as TSLP.
TSLP has helped transform the scientific picture of allergic disease. Instead of beginning the story with an immune system that inexplicably attacks harmless substances, researchers can now ask an earlier question: What happened at the barrier that convinced the immune system there was danger?
The answer may help explain not only why allergy begins, but also why inflammation that appears to start in one organ can sometimes be followed by disease in another.
The Immune System’s Border Patrol
Every day, the body performs an extraordinary act of biological discrimination. The intestine encounters kilograms of food and houses trillions of microorganisms, yet most of these interactions do not produce destructive inflammation. The lungs continuously filter enormous volumes of air containing particles, microbial fragments and environmental chemicals. The skin is exposed to friction, ultraviolet radiation, microbes, detergents and allergens.
An immune system that attacked everything would make ordinary life impossible. Barrier tissues therefore do much more than separate inside from outside. They help determine which encounters should be ignored, which should be tolerated and which should trigger defense.
TSLP is one of the signals involved in that decision. Produced largely by epithelial cells, TSLP can be released in response to tissue disturbance and inflammatory signals. Once present, it acts on a surprisingly broad network of immune cells. Dendritic cells are among its most important targets, but basophils, mast cells, eosinophils and T cells can also respond directly or indirectly to its influence.
The consequence is often a shift toward type 2 immunity. Evolution did not invent type 2 immunity to make people allergic to cats or pollen. This ancient defense program helps protect against large parasites and participates in tissue repair. It promotes mucus production, recruits specialized immune cells and alters the behavior of tissues exposed to injury.
But an immune program built for parasites and damaged tissues can become destructive when repeatedly directed against harmless environmental substances. That is where the biology of TSLP becomes especially revealing.
How a Harmless Particle Becomes an Immune Threat
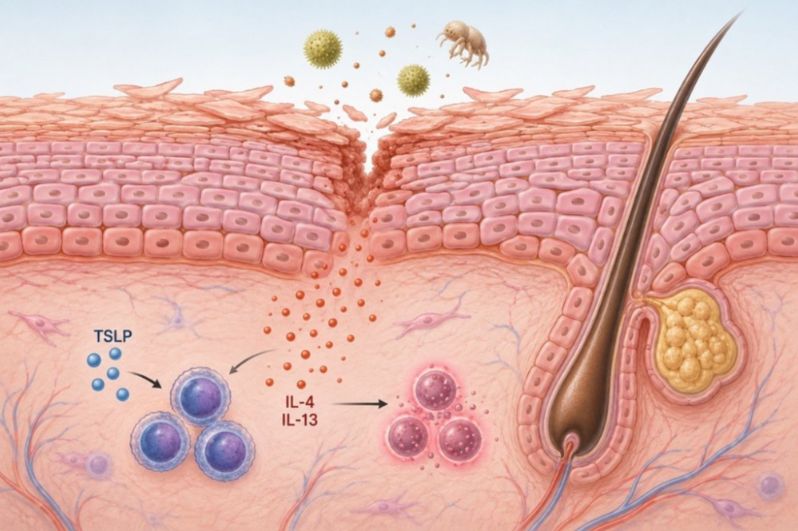
Imagine an allergen reaching the airway surface. The allergen itself may not be inherently dangerous. But some environmental allergens contain proteases, enzymes capable of cutting proteins, or other components that disturb epithelial cells and barrier integrity. The tissue senses disruption.
The alarm begins locally. Epithelial cells release TSLP and other warning signals. Nearby dendritic cells receive the message. These dendritic cells then change how they communicate with T cells, increasing signals that favor a type 2 immune response while reducing signals that would push immunity in competing directions.
The dendritic cell is no longer merely carrying an allergen to the immune system. It is carrying the allergen with instructions. Those instructions matter. Under the influence of TSLP, dendritic cells increase OX40 ligand, a molecule that helps guide T cells toward a type 2 inflammatory identity. They also produce chemokines that attract additional immune cells into the developing response.
Basophils can contribute signals such as interleukin-4. Mast cells can amplify tissue inflammation. Eosinophils can accumulate at inflammatory sites. T cells can sustain and organize the response. A small disturbance at the epithelial surface has become an immune network.
With repeated exposure, the network can become persistent. The result may be chronic itching in the skin, mucus and airway narrowing in asthma, or recurrent inflammation at other barrier surfaces. From this perspective, allergy is not simply a mistaken antibody response. It is a breakdown in communication between the environment, the barrier and the immune system.
The Skin May Be Talking to the Lungs
One of the most intriguing implications of barrier immunology is that inflammation may not always remain confined to the tissue where it begins. Children with atopic dermatitis are more likely than other children to later develop food allergy, allergic rhinitis and asthma. This sequence is often called the atopic march.
The traditional description is chronological: eczema appears first, then other allergic diseases follow. But chronology does not explain mechanism. TSLP offered researchers a possible biological bridge.
In experimental models, excessive production of TSLP in the skin can produce eczema-like inflammation. More provocatively, high levels of skin-derived TSLP can influence inflammatory responses in the lungs.
The implication is not that every case of childhood eczema inevitably causes asthma. The atopic march is biologically diverse, and genetics, allergen exposure, infections and other epithelial signals all contribute. But the experiments introduced a powerful concept: a damaged barrier in one organ may send signals with consequences beyond that organ.
The skin may not be an isolated battlefield. It may be an entry point into a broader inflammatory state. This possibility is especially visible in Netherton syndrome, a rare inherited disorder involving severe skin-barrier dysfunction and profound allergic disease. In this condition, genetic disruption leads to uncontrolled activity of enzymes in the skin. Those enzymes activate signaling pathways in keratinocytes, the major cells of the epidermis, driving TSLP production.
The sequence is unusually clear: a genetic defect alters the barrier, the disturbed barrier produces an immune alarm signal, and severe allergic inflammation follows. For more common allergic diseases, the pathways are unlikely to be so simple. Yet the principle may be similar. Barrier disturbance comes first. Immune instruction follows.
The Lung Is Not Just a Target
Asthma has often been described as a disease of immune cells infiltrating the lungs. That description is correct but incomplete. The airway lining itself is an active participant. The respiratory epithelium is exposed continuously to viruses, allergens, smoke, particulate pollution and chemical irritants. When epithelial cells detect injury or inflammatory signals, they can release TSLP and other alarm molecules.
This means the lung is not merely the place where allergic inflammation happens. It can help initiate and organize that inflammation. Respiratory viruses provide an important example. Viral infections can disturb the airway epithelium and alter the local immune environment. Research reviewed by Ziegler and Artis suggested that respiratory syncytial virus, or RSV, can induce TSLP production, potentially encouraging type 2 inflammatory responses associated with childhood wheezing and asthma.
The sequence raises a larger question. Could repeated environmental injuries, viral infections, allergens, pollutants and other irritants, repeatedly activate the same epithelial alarm systems?
If so, chronic allergic disease may sometimes represent the accumulated biological memory of repeated barrier disturbance. The immune system does not encounter the environment directly. It often encounters the environment through the interpretation of epithelial tissues. And those tissues may remember trouble.
One Molecule, Two Very Different Outcomes
TSLP is not inherently harmful. That is one of the most important lessons of its biology. In the intestine, epithelial TSLP appears to participate in maintaining a relatively peaceful relationship with the enormous microbial population living there. The gut must defend against pathogens while tolerating food and commensal organisms. TSLP can help shape dendritic cells toward less inflammatory behavior and may support regulatory immune responses.
Animal studies have found that disrupting TSLP signaling can worsen some forms of intestinal inflammation. Altered TSLP expression has also been observed in the intestinal tissue of people with Crohn’s disease.
How can the same molecule contribute to tolerance in one setting and allergy in another? Because the immune system is contextual.
A cytokine does not carry a single universal meaning. Its effects depend on the tissue in which it appears, the other signals present at the same time, the cells available to respond and the duration of exposure.
In the gut, TSLP may help maintain coexistence. In a damaged airway repeatedly exposed to allergens, it may help sustain asthma. In inflamed skin, it may contribute to eczema and possibly influence immune responses elsewhere.
The biology resists the simple division of immune molecules into “good” and “bad.” TSLP is better understood as a coordinator of barrier immunity, a system that can preserve health or drive disease depending on the circumstances.
Real Danger and Mistaken Danger
The evolutionary logic of TSLP becomes clearer when considering parasitic worms. Large parasites cannot be eliminated in the same way as bacteria. They require a different type of immune strategy, one involving mucus production, tissue changes and type 2 immune responses. In some helminth infections, TSLP helps create the conditions necessary for this response by suppressing competing inflammatory pathways.
In that setting, the alarm makes sense. The body detects tissue disturbance associated with a genuine biological threat and launches a defense program suited to the problem.
Allergy may use much of the same machinery against the wrong target. A pollen grain is not a worm. A dust mite protein is not invading tissue in the manner of a parasite. Yet allergens can disturb epithelial surfaces and activate molecular pathways that resemble those triggered by injury or infection.
The barrier sounds the alarm. The immune system responds to the alarm. And the resulting inflammation can become more damaging than the original exposure.
This helps explain why describing allergy simply as an “overactive immune system” can be misleading. The immune response may be highly organized and biologically coherent. The problem is that a protective program has been activated in an inappropriate context, perhaps repeatedly, until it becomes chronic disease.
From Local Allergy to Systemic Inflammation
The emerging science of barrier immunity also raises a broader possibility: diseases that appear anatomically separate may be biologically connected. The skin, lungs and gastrointestinal tract are structurally different organs, but they share an important feature. All are epithelial interfaces with the outside world.
All can sense environmental change. All can produce immune signals. And all communicate with circulating immune cells capable of moving between tissues. TSLP is unlikely to explain every connection among allergic diseases, and it should not be treated as a single master switch controlling all systemic inflammation. The immune system is far more complex. Other epithelial alarm signals, including IL-25 and IL-33, participate in overlapping networks, and genetics, microbiomes, infections and environmental exposures shape the outcome.
Still, TSLP helped establish a crucial framework. A disease that appears in the skin may begin with more than a skin problem. Airway inflammation may involve more than the lungs. Intestinal immune disturbances may reflect changes in how the barrier communicates with microbes and immune cells.
The body’s barriers form an interconnected immunological system. From this perspective, the familiar categories of eczema, allergic rhinitis and asthma may represent different expressions of disturbed communication at environmental interfaces rather than completely independent diseases. That possibility is reshaping both research and treatment.
Treating the Alarm, Not Just the Aftermath
For decades, many allergy treatments focused primarily on controlling the consequences of inflammation: blocking histamine, relaxing airway smooth muscle, suppressing immune activity with corticosteroids or targeting downstream inflammatory molecules.
The discovery of TSLP biology suggested another strategy. What if treatment could interrupt the alarm signal closer to the beginning of the inflammatory cascade?
Because TSLP acts upstream of multiple immune-cell pathways, blocking it has the potential to affect several components of type 2 inflammation simultaneously. The concept emerging from early barrier-immunity research has since become clinically important, reinforcing the idea that epithelial signaling is not merely an academic curiosity but a therapeutically meaningful part of allergic disease.
The deeper lesson extends beyond any single drug target. Allergy may begin earlier than scientists once thought. Before the IgE antibody attaches to a mast cell, before the eosinophil enters the tissue and before the airway begins to tighten, there may be a conversation taking place at the body’s surface.
A cell lining the skin, lung or intestine senses disturbance. It releases an alarm. The immune system listens. And whether that conversation ends in protection, tolerance or chronic disease may depend on what the barrier says next.
Reference
1. Ziegler SF, Artis D. Sensing the outside world: TSLP regulates barrier immunity. Nat Immunol. 2010;11(4):289-293. doi:10.1038/ni.1852
2. Soumelis V, Reche PA, Kanzler H, et al. Human epithelial cells trigger dendritic cell mediated allergic inflammation by producing TSLP. Nat Immunol. 2002;3(7):673-680. doi:10.1038/ni805
3. Ito T, Wang YH, Duramad O, et al. TSLP-activated dendritic cells induce an inflammatory T helper type 2 cell response through OX40 ligand. J Exp Med. 2005;202(9):1213-1223. doi:10.1084/jem.20051135
4. Ying S, O'Connor B, Ratoff J, et al. Thymic stromal lymphopoietin expression is increased in asthmatic airways and correlates with expression of Th2-attracting chemokines and disease severity. J Immunol. 2005;174(12):8183-8190. doi:10.4049/jimmunol.174.12.8183
5. Demehri S, Morimoto M, Holtzman MJ, Kopan R. Skin-derived TSLP triggers progression from epidermal-barrier defects to asthma. PLoS Biol. 2009;7(5):e1000067. doi:10.1371/journal.pbio.1000067